
Distributed Antenna Systems in Healthcare (Hospital DAS Guide)
Hospitals are designed to provide care. Most are not designed to pass cellular signals.
Reinforced concrete, steel infrastructure, energy-efficient glass, and shielded imaging rooms weaken carrier coverage. At the same time, healthcare operations depend heavily on mobile communication, creating a gap between clinical mobility needs and wireless performance.
A Distributed Antenna System, commonly called DAS, helps close that gap. This guide explains what DAS means in a healthcare setting, why it matters for public cellular coverage, and how hospital leaders should approach solution selection.
Key Takeaways
A Distributed Antenna System (DAS) improves indoor cellular coverage throughout hospitals and healthcare facilities.
Healthcare DAS supports reliable communication for clinicians, patients, and emergency responders.
Modern hospital DAS deployments typically connect directly to mobile network operators through fiber backhaul into headend radio equipment.
Hospitals often deploy DAS alongside enterprise WiFi to support both carrier connectivity and internal network applications.
Proper DAS design requires RF assessment, carrier coordination, and planning for future wireless growth.
What Is a DAS in a Healthcare Setting?

A Distributed Antenna System (DAS) in healthcare is an in-building wireless network that captures cellular signal and redistributes it through a network of indoor antennas to provide consistent coverage throughout a hospital or medical campus.
Hospitals often experience weak cellular signal due to reinforced concrete, steel infrastructure, and shielded medical imaging areas. A DAS distributes carrier signal evenly across the facility to eliminate these coverage gaps.
In simple terms, a DAS brings outdoor cellular signal indoors and distributes it across the building to support reliable communication for clinicians, patients, and emergency responders.
Healthcare DAS supports:
Voice calls and SMS
Secure clinical messaging apps
4G LTE and 5G connectivity
Public safety radio systems
Cellular-connected IoT devices
Hospitals often struggle with dead zones in stairwells, basements, emergency departments, and imaging areas. A properly designed DAS eliminates those coverage gaps.
Why Healthcare Facilities Need DAS

Patient Safety and Communication
Clear communication directly impacts patient outcomes. Care teams coordinate across departments in real time, and unreliable cellular coverage can disrupt those workflows. Reliable indoor signal ensures clinicians can communicate when seconds matter.

Clinical Mobility
Healthcare professionals move constantly between patient rooms, departments, and floors. Mobile communication tools allow clinicians to coordinate care efficiently. Strong cellular coverage supports these mobile workflows across the entire facility.
Patient and Visitor Connectivity
Patients and visitors increasingly rely on mobile connectivity for communication, telehealth access, and digital health tools. Reliable cellular service improves the overall healthcare experience and supports modern hospital operations.
Types of DAS Used on Hospitals
Hospitals deploy several types of Distributed Antenna Systems depending on facility size, capacity requirements, and long-term scalability needs.
Active DAS
Active DAS uses fiber optic infrastructure to distribute cellular signal to remote radio units located throughout the hospital. These systems support multiple wireless carriers and handle high device density, making them ideal for large hospitals and multi-building medical campuses.
Passive DAS
Passive DAS distributes cellular signal using coaxial cabling and passive signal splitters. These systems are typically deployed in smaller healthcare facilities where coverage needs are more limited and device density is lower.
Hybrid DAS
Hybrid DAS combines fiber backbone infrastructure with coaxial signal distribution. This approach balances scalability and cost, making it a practical solution for mid-sized hospitals or healthcare facilities planning for future wireless growth.
Selecting the right DAS architecture depends on building size, wireless demand, and long-term scalability requirements.
Signal Sources for Healthcare DAS
A DAS does not create cellular signal. It distributes signal from a source. Selecting the right signal source is as important as choosing the DAS architecture.
Two signal source options prevail:
Off‑Air Repeaters /
Bi‑Directional Amplifiers (BDAs)
These solutions capture existing outdoor carrier signal and amplify it indoors before distribution through the DAS.
Pros: Faster deployment when strong outdoor signal exists, lower infrastructure requirements.
Cons: Dependent on macro network quality, limited scalability in dense environments.
Carrier‑Provided Radio Base Stations
In this model, one or more mobile operators provide dedicated radio base stations (or small cell nodes) inside the building. Products such as compact radio platforms (for example, solutions like CTS Forte) act as a direct, controlled signal source that feeds the DAS.
Pros: High-quality, predictable signal with strong 5G support and better performance in mission-critical environments.
Cons: Requires deeper carrier coordination and longer planning cycles.
Think in two layers:
Signal source: where and how cellular signal is generated or brought inside.
DAS: how that signal is distributed throughout the facility.
Both layers must align to meet coverage, capacity, and multi-carrier objectives.
Hospital Distributed Antenna System (DAS) Architecture
A healthcare DAS uses a central signal source and in-building distribution network to deliver consistent cellular coverage throughout a hospital.
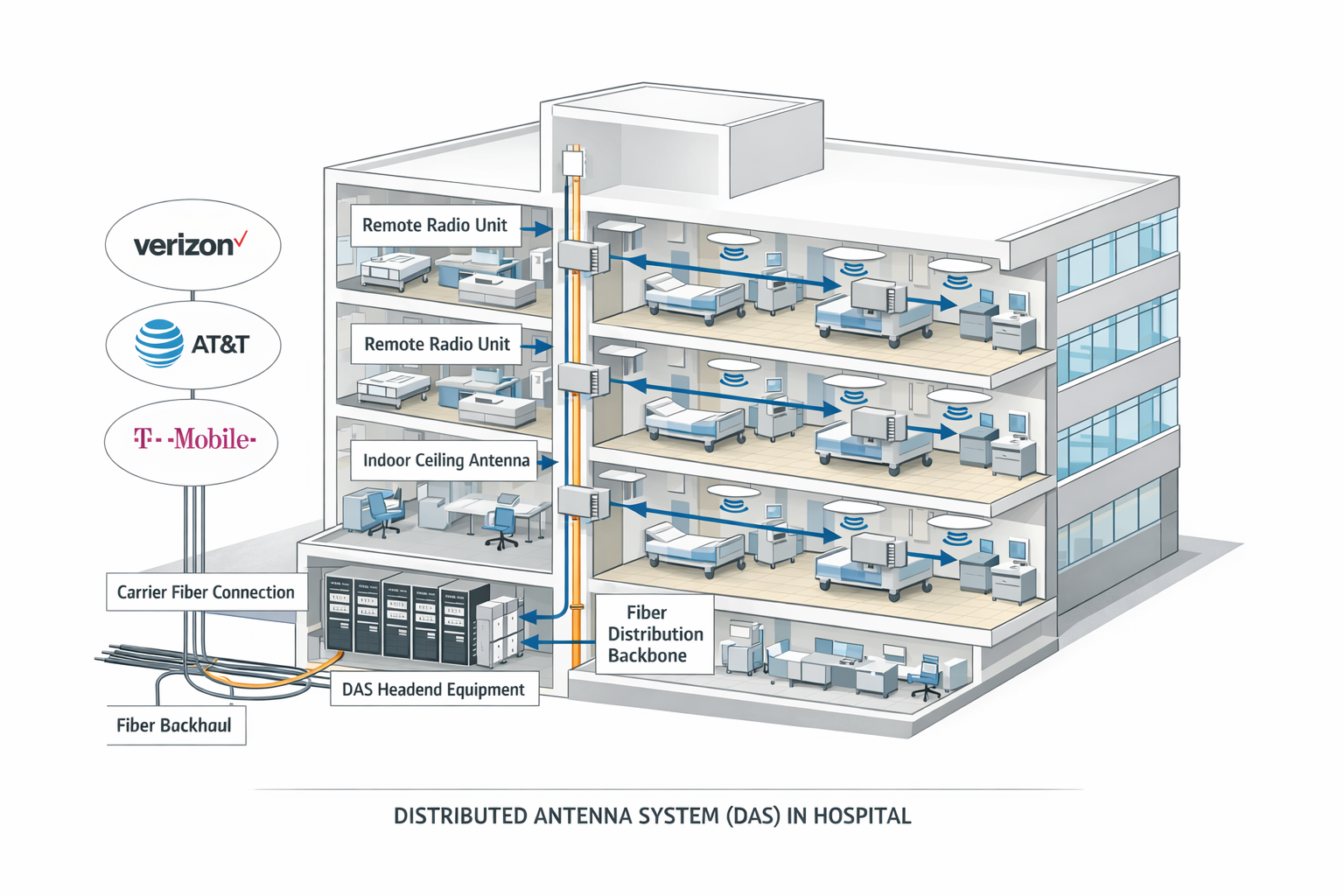
Figure: Example hospital distributed antenna system architecture
Core Components of a Healthcare DAS
Signal Source
Carrier signal enters the facility from the external network (often via a nearby macro network or a dedicated signal source).
Headend Equipment
The headend processes and conditions the signal before it is distributed throughout the hospital.
Distribution Network
Fiber optic cabling (active/hybrid) or coaxial cabling (passive) transports signal across floors and buildings.
Remote Units
Remote radio units deliver conditioned signal closer to coverage areas and support capacity in high-demand zones.
Indoor Antennas
Ceiling-mounted antennas provide consistent coverage in patient rooms, corridors, stairwells, basements, and critical departments.
Hospitals often require special planning for infection control, shielding in imaging areas, and public safety radio coverage testing. These factors should be accounted for early in DAS design and deployment.
In-Building Cellular Architectures for Healthcare
Hospitals can deploy several types of in-building cellular architectures. Distributed antenna systems (DAS) remain the most common approach for large hospitals and medical campuses, but alternatives such as small cell systems and CBRS-based neutral host networks are increasingly evaluated depending on facility size, carrier requirements, and long-term wireless strategy.
Distributed Antenna Systems (DAS)
A Distributed Antenna System distributes cellular signal from a centralized signal source through a network of indoor antennas across the facility.
DAS is typically selected for:
Large acute-care hospitals and medical centers
Environments requiring multi-carrier support on standard smartphones
High-density areas such as emergency departments, operating rooms, and lobbies
For many healthcare systems, DAS remains the most predictable architecture for carrier-grade indoor coverage across large or complex facilities.
Small Cells and MORAN
Small cell systems use low-power cellular radios placed throughout the facility. In a Multi-Operator Radio Access Network (MORAN) configuration, a single small cell platform can support multiple carriers on a shared radio layer.
Hospitals may consider small cell architectures when:
They are building or renovating with a strong IP networking foundation
They want an architecture that behaves more like a “cellular LAN”
Coverage areas are more contained or modular
Because MORAN represents a different design model, healthcare IT leaders should evaluate it side-by-side with DAS with help from advisors who understand both approaches.
CBRS-Based Neutral Host (MOCN)
CBRS (Citizens Broadband Radio Service) allows hospitals to deploy their own LTE or 5G radios using shared spectrum and connect into mobile operator networks through a Multi-Operator Core Network (MOCN) model.
This approach may be considered when:
Organizations are exploring private cellular or advanced IoT deployments
There is alignment with specific carrier roadmaps
The hospital is planning long-term wireless transformation
However, support from major carriers for CBRS neutral host remains limited and evolving, so it is often viewed as a future-oriented strategy rather than a primary solution for immediate multi-carrier coverage.
Voice over Wi-Fi and Wi-Fi First
Voice over Wi-Fi (Wi-Fi Calling) allows mobile devices to route voice and data traffic over a Wi-Fi network instead of the cellular network.
Technologies such as Passpoint and OpenRoaming allow devices to authenticate automatically to Wi-Fi networks.
While Wi-Fi-based approaches can strengthen connectivity in areas with strong wireless LAN coverage, they typically do not replace the need for a dedicated in-building cellular architecture to support all carriers and devices across a hospital campus.
How to Decide
A practical decision framework for healthcare IT leaders:
Define primary objectives such as multi-carrier support and critical coverage zones.
Select one primary architecture that aligns with risk tolerance and long-term strategy.
Choose the appropriate signal source model for that architecture.
Validate assumptions with experienced advisors who understand DAS, small cells, and CBRS options.
Architecture and signal source selection should be driven by hospital needs, not by a single vendor’s product portfolio.
| Architecture | Best For | Multi-Carrier Support | Scalability |
|---|---|---|---|
| DAS | Large hospitals and multi-building campuses | Excellent | Very high |
| Small Cells / MORAN | Facilities with strong IP networking foundations | Good | Moderate |
| CBRS Neutral Host | Private LTE / 5G and advanced IoT strategies | Limited today | High future potential |
| Wi-Fi Calling | Supplemental indoor coverage | Device dependent | Limited |
DAS vs WiFi in Healthcare
A common misconception in healthcare environments is that improved WiFi coverage can replace a Distributed Antenna System. In reality, DAS and WiFi serve different purposes and support different types of wireless communication.
Hospitals require both systems working together to support clinical operations, mobile communication, and patient connectivity.
| Capability | DAS | WiFi |
|---|---|---|
| Carrier cellular coverage | Supported | Not Supported |
| Voice calls and SMS | Supported | Limited |
| Supports mobile carrier networks | Supported | Not Supported |
| Internal hospital applications | Not Supported | Supported |
| Electronic health record access | Not Supported | Supported |
| Guest internet access | Not Supported | Supported |
| Works without hospital network login | Supported | Not Supported |
DAS distributes licensed cellular spectrum from mobile carriers and ensures reliable indoor signal throughout a healthcare facility. WiFi supports internal hospital networks, including electronic health records, VoIP systems, and guest internet access.
Because they serve different roles, most hospitals deploy both DAS and enterprise WiFi infrastructure to support modern healthcare operations.
Key Design Considerations
Designing a Distributed Antenna System for a hospital environment requires careful planning to ensure reliable coverage, regulatory compliance, and long-term scalability.

RF Assessment
Every healthcare facility has unique construction materials and structural layouts that impact wireless signal propagation. A predictive RF study identifies coverage gaps and determines optimal antenna placement throughout the hospital.

Scalability for 5G and Private Networks
5G adoption continues to expand in healthcare for imaging, telemetry, and advanced applications. In‑building systems should support future spectrum bands and architectures (including CBRS for private 5G) without requiring full replacement.

Carrier Coordination
Carrier participation influences timeline and system configuration. Early engagement with mobile operators, or a neutral host partner, reduces delays and helps align on technology choices.
Infection Control Planning
Healthcare environments require strict construction protocols. Installation must align with infection control risk assessments to avoid disruption to patient care areas.
Benefits of Implementing DAS in Healthcare
A properly designed Distributed Antenna System improves communication reliability, regulatory compliance, and long-term wireless infrastructure performance across healthcare facilities.
Improved Communication Reliability
Stronger indoor signal reduces dropped calls and improves message delivery consistency for clinicians, staff, patients, and visitors.
Operational Efficiency
Mobile workflows function more smoothly when connectivity is stable. Teams can rely on a single device for voice, secure messaging, alerts, and clinical apps as they move throughout the facility.
Long-Term Infrastructure Value
Scalable systems reduce the need for costly retrofits as wireless demand grows and as hospitals explore private 5G.How long does a Hospital DAS deployment take?
Deployment timelines vary depending on facility size, carrier approvals, chosen architecture, and construction phasing.
Mid-sized hospital projects often require several months from assessment to final validation. Early planning improves execution speed by aligning stakeholders, technology choices, and construction schedules.
Typical DAS Deployment Phases
RF Assessment and System Design
Engineers conduct predictive modeling and on-site testing to determine antenna placement and system architecture.Carrier Coordination and Approvals
Mobile network operators review the system design and coordinate integration with their networks.Installation and Infrastructure Buildout
Fiber, cabling, remote units, and antennas are installed throughout the hospital while following infection control protocols.Testing and Optimization
Engineers perform coverage testing and system optimization to ensure reliable signal levels across the facility.
Early planning and coordination between hospital facilities teams, IT departments, and DAS integrators can significantly improve project timelines and deployment efficiency.
Frequently Asked Questions
-
DAS stands for Distributed Antenna System. It is an in-building wireless infrastructure that distributes cellular signal throughout a hospital or healthcare facility to provide reliable indoor coverage for mobile devices and communication systems.
-
In many jurisdictions, hospitals must meet Emergency Responder Radio Coverage (ERRC) requirements defined by local fire codes. These regulations ensure that first responders can maintain radio communication inside buildings. A DAS is often used to meet these coverage requirements.
-
Yes. Modern active and hybrid DAS platforms are designed to support both 4G LTE and 5G frequency bands. Systems can often be upgraded to support additional spectrum as mobile carriers expand their networks.
-
No. DAS and WiFi serve different purposes. DAS distributes licensed cellular spectrum from mobile carriers, supporting voice calls, SMS, and carrier-based applications. WiFi supports internal hospital networks, such as electronic health records, VoIP systems, and guest internet access.
Most hospitals deploy both systems together to support clinical communication and data access.
-
Indoor DAS antennas are usually mounted in ceilings throughout patient rooms, hallways, stairwells, basements, emergency departments, and other areas where cellular coverage may be weak.
Proper antenna placement is determined through an RF assessment and system design process.
-
Most modern hospital DAS deployments connect directly to mobile network operators through fiber backhaul into the DAS headend equipment, where carrier radios distribute signal through the building. This architecture provides more reliable performance than off-air donor antenna systems.
Future Outlook for Healthcare DAS
Healthcare environments are becoming increasingly connected as mobile health platforms, IoT devices, and real-time clinical communication tools expand across hospitals and medical campuses.
Reliable in-building wireless infrastructure will continue to play a critical role in supporting these technologies and ensuring consistent connectivity for clinicians, patients, and emergency responders.
Over the next several years, healthcare wireless infrastructure is expected to evolve in several important ways:
Greater adoption of 5G across healthcare campuses
Mobile carriers continue expanding 5G services, increasing the demand for in-building infrastructure that supports new spectrum bands.Higher device density inside hospitals
Connected medical devices, mobile workstations, and IoT sensors are increasing the number of wireless devices operating inside healthcare facilities.Stronger enforcement of public safety coverage requirements
Many jurisdictions are tightening enforcement of Emergency Responder Radio Coverage standards for hospitals and other critical facilities.Closer collaboration between IT and facilities teams
Wireless infrastructure planning increasingly involves coordination between hospital IT departments, facilities teams, and telecommunications providers.
Hospitals are evolving into fully connected digital environments. Scalable wireless infrastructure, including Distributed Antenna Systems, will be essential to supporting the next generation of healthcare communication and technology.
Final Takeaway
Hospitals rely on constant communication between clinicians, support staff, patients, and emergency responders. When cellular coverage is inconsistent inside a healthcare facility, communication delays and workflow disruptions can occur.
A well-designed Distributed Antenna System ensures reliable indoor cellular connectivity throughout the hospital environment. By supporting mobile communication, meeting public safety coverage requirements, and providing scalable infrastructure for future technologies, DAS plays a critical role in modern healthcare facilities.
When evaluating in-building wireless solutions, hospitals should focus on long-term reliability, regulatory compliance, and infrastructure that can adapt to growing wireless demand. Thoughtful planning and proper system design help ensure that connectivity supports the mission of delivering high-quality patient care.
Reliable in-building wireless infrastructure helps healthcare organizations maintain the communication systems that modern patient care depends on.
Related Resources
Healthcare Connectivity Solutions
Explore in-building wireless solutions designed to improve cellular coverage across healthcare environments.
Distributed Antenna Systems Overview
Learn how DAS technology delivers reliable cellular connectivity inside large buildings and complex facilities.
Understand how public safety distributed antenna systems support first responder communications inside buildings.
Why Cellular Coverage in Hospitals Is Failing
Learn why hospitals often struggle with weak indoor cellular signal and how building materials affect wireless coverage.
How Hospitals Are Solving Cellular Coverage Problems with DAS and Private Networks
Explore the technologies hospitals are deploying to deliver reliable connectivity across healthcare campuses.
Planning a Healthcare DAS Deployment?
Designing in-building cellular infrastructure for hospitals requires coordination between RF engineering, healthcare construction planning, and mobile network operators.
CTS provides vendor-neutral design, deployment, and lifecycle support for hospital DAS, small cell, and private cellular architectures.
If you're evaluating cellular coverage for a healthcare facility or medical campus, our wireless architects can help.
CTS designs and deploys healthcare DAS systems for hospitals and medical campuses across the United States.